This Journal considers how the practice of medicine has changed in the post WWII period.
I have reprinted an article by writer Sheramy Tsai who has written a large collection of very excellent health related articles, all of which I heartily recommend.
At the end of her article I have registered some special anecdotes about a great physician I have known, and then a few personal comments.
The article below appeared in The Epoch Times on February 7, 2026. This publication offers some of the best and most applicable health related writing you may ever encounter. The health articles are simply written, direct, balanced and research based.
I’ll keep posting relevant health articles from The Epoch Times. I’ll also post articles from other informative contributors, such as Dr. Joseph Mercola, D.O., The Midwestern Doctor, and Dr. James Roach, M.D. in Midway, Kentucky.
Dr. Joseph Mercola has been writing good health articles for 30 years. He publishes 3 articles daily, plus relevant news briefs. The anonymous Midwestern Doctor publishes the most exhaustive, well researched, and well written articles you will ever encounter in his Substack offering The Forgotten Side of Medicine. Dr. Roach puts out a monthly collection of pertinent research articles on common health subjects from his clinic, The Midway Center for Integrative Health.
These 4 broad sources of health information are my top of the line. Any one of these sources will keep you well informed with actionable and reliable information.
Let’s consider just a few sobering statistics about health care in America.
U.S. health care spending reached $5.3 trillion in 2024, according to recently released data from the Department of Health and Human Services. That includes all health spending through federal and state health programs like Medicare and Medicaid, money paid by individuals to health insurers and providers, spending by employers, and payments made by insurance companies.
At $15,000 a person (!) the United States has the highest per capita spending in the world. In 2024 it was nearly 50 percent higher than the next highest country, Switzerland, which spends $10,000 per citizen. The U.S. is an outlier in health care spending.
How did America wind up spending the most in the world on health care, and at the same time rank in the mid range (or lower) of countries for the true health and happiness of its citizens?
Let’s have a look at Sheramy Tsai’s fine writing. Perhaps some clues about the current state of American health are to be found here.
What American Medicine Lost in the Past 50 Years

Patients came by train from Brooklyn, and Dr. Felix “Big Frank” Ittleman picked them up at the station, treated them in the parlor, then drove them back. “People said talking to him was like talking to a priest,” his son, Frank Ittleman, told The Epoch Times. “Only better.”

Dr. Felix Ittleman on a winter house call in Great Neck, N.Y., circa 1950. Photo provided by Frank Ittleman.
The medicine of that era saved fewer lives, but it held a kind of attention that shaped the encounter. Doctors listened without rushing and sensed the worries behind a patient’s words—what Ittleman would later call “the complexities of the soul.” Presence was part of the diagnostic tool kit, not an afterthought.
As care shifted into larger systems, the work changed. Payment began to reward what could be coded rather than the time spent understanding a patient. Technology expanded what was possible, yet connection narrowed. Visits shortened. Familiar faces disappeared. The small cues that once guided a diagnosis grew easier to miss.
The result was progress with a missing piece. Doctors who once crossed blizzards to reach patients now struggle to reach them through an avalanche of screens, rules, and codes.
Some physicians are trying to bring those elements back together, pairing the precision of modern medicine with the attention that once anchored care, an effort to restore the one thing both patients and doctors have steadily lost: time.
How Everyday Care Was Rebuilt for Speed
By the time Ittleman entered medicine in the 1970s, the world that shaped his father was already fading.
One of the quiet drivers of that shift has been the erosion of primary care. Over several decades, fewer physicians entered or remained in generalist roles, even as patients lived longer with more chronic and complex illnesses. Primary care physicians, the clinicians best positioned to integrate symptoms, context, and care over time, became harder to find.
As primary care thinned, the system adapted to its absence. Patients without a primary doctor moved between urgent-care centers and emergency rooms, specialists, and hospital networks. Responsibility fragmented. Medicine grew more capable, but less anchored.
What that anchor once looked like is still vivid to those who lived inside it.
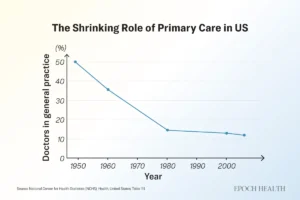
The share of U.S. physicians working in general practice and family medicine has steadily declined since the mid-20th century.
The Continuity That Once Defined Care
Brian Harwood remembers evenings in the 1950s when neighbors crowded the hallway of his family’s home in Waterbury, Vermont, waiting to see his father, Dr. Charles Harwood, without appointments. “People would just come and wait,” he told The Epoch Times. “He never rushed a patient.”
The elder Harwood mixed his own medicines and poured cough syrup from five-gallon jars, then headed out in deep winter when calls came—sometimes by sleigh, sometimes in a car fitted with snow tracks. When cash was tight, payment might be a jar of quarters or a side of beef.
For many who lived through that era, feeling cared for began with being known. As a child in the 1960s, Susan Hooper, now 73, remembers her pediatrician, Raymond “Doc” Towne, vaccinating classmates at school and treating every sore throat. Patients walked in expecting to be seen that day by someone who knew them, sometimes, quite literally, from birth.
Her experience today looks different. Hooper told The Epoch Times she recently waited seven months for a spinal ablation—a procedure that did not exist in her childhood and no neighborhood doctor could have performed. But the wait, at a short-staffed clinic later absorbed into a larger network, highlighted something else that had thinned: the sense of being known. “You don’t call and have someone know who you are anymore,” she said. “That’s different.”
As small practices have closed or been absorbed into bigger systems, that thread has frayed. Patients now move among rotating clinicians, urgent-care sites, and specialists—a model that broadens access to expertise but often scatters the relationships that once grounded care. Records follow patients; relationships rarely do.
Continuity never guaranteed perfect care, but its absence changed the feel of medicine—when a visit begins not with recognition but with the need to explain yourself all over again.
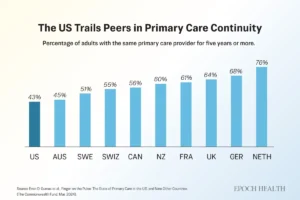
Fewer than half of U.S. adults report having the same primary care provider for five years or more, trailing most peer nations.
Lost Skills That Once Anchored Care
Ittleman uses skills that younger doctors may learn, but rarely have time to develop. He sits at eye level, rests a hand on a shoulder, or waits long enough for a patient’s real concern to surface. “I never hesitate to touch a patient,” he said. “That’s how you understand someone. That’s how you build trust.”
The physical exam has drifted in the same way. A skilled clinician can still catch what machines miss—subtle swelling, a change in breathing, unease in a patient’s eyes—but its deeper value lies in human contact, in making room for fears patients struggle to name. That kind of listening takes time, a resource clinicians have the least of.
“We don’t set aside the time to talk to patients, to find out what really makes them tick,” Ittleman said. The result, he added, is not a loss of compassion, but a loss of the conditions that allow it to function.
Ittleman worries about what’s lost when AI drafts visit notes. To him, the medical record was never just documentation; it was a record of a relationship. “The note is precious,” he said. “It should reflect the intimacy of what happened in that room, not just the codes.”
He holds onto that ethic in small ways. When patients die, he writes handwritten letters to their families, explaining what happened and acknowledging any uncertainty or error. For many families, those letters become part of the healing.
To Ittleman, the erosion of listening and touch carries a cost that cannot be measured on a monitor. “Doctors today,” he said, “have lost the ability to deal with the complexities of the soul.”
The Part Nostalgia Leaves Out
For all the warmth in those memories, mid-century medicine was far from idyllic. Pacemakers were the size of car batteries. Syringes were reused until their needles dulled. Heart attacks were often fatal. Many cancers were found only after they had spread. Infant and maternal deaths were far higher. Life expectancy at mid-century was nearly a decade shorter than it is today.
Hooper knows that gap firsthand. When she was an infant, her mother grew exhausted and lost weight, symptoms doctors initially dismissed as the strain of caring for four children. Exploratory surgery later revealed advanced cancer throughout her abdomen. She died months later. “I do wonder if, with health care like it is today,” Hooper said, “something would have been picked up sooner.”
Ittleman is quick to push back on any rose-colored view of his father’s era. Care was compassionate, he said, but profoundly constrained. “You have to remember what we couldn’t do. We didn’t have the drugs, the imaging, the operations we have now.”
Over four decades in cardiac surgery, he watched those tools transform what was possible. Patients who would not have survived his father’s time now went home to their families. “Medicine has become incredibly sophisticated,” he said. “What we can offer now is monumental compared with what my father had.”
The risk, he said, is not that progress went too far, but that in making room for everything medicine can do, the system crowded out the parts of care that never depended on technology. It is possible to save more lives and still lose something essential in the process.
The Quiet Return
If the past cannot be reclaimed, the question becomes whether its most human elements can be reassembled inside modern medicine.
Across the country, physicians are quietly rebuilding care around time. In direct primary care practices, patients pay a monthly fee in place of insurance for routine services. In concierge medicine, an annual retainer supports smaller patient panels.
In both models, doctors see fewer patients and spend more time with each one. Same-day appointments are common. Communication is often direct. Early studies link these approaches to fewer emergency visits, stronger continuity, and lower rates of clinician burnout.
Costs vary widely, from modest monthly payments—sometimes under $75—to higher-end retainers. Their appeal reflects a growing willingness to trade breadth for time, continuity, and access.
One of those patients is Sandy Lawrence, an 81-year-old Houston woman who told The Epoch Times that she spent years feeling rushed through traditional care. She now pays a yearly fee to stay with her internist, has her cellphone number, and hears back quickly. “It’s like having a doctor who actually has time again,” she said.
Ittleman distills that ethic for his trainees into four sentences that he considers more enduring than any device: I made a mistake. I’m sorry. I don’t know. I will find out.
“If you can say those honestly,” he said, “you’ll be a good doctor, no matter what technology you have.”
Taken together, these efforts look less like a return to the past than a recalibration. Modern medicine will continue to advance, but the parts of care patients remember most—being known, being heard, and being cared for—still depend on time, presence, and attention.
That may be the clearest path back to healing.”
Crestone and Beyond
I want to write a bit about a great physician, and share with you just a few anecdotes about her life and her style of medical practice.
I was born to physician parents. My father was a general surgeon and my mother was an internist. Both received excellent training in the 1930s and 1940s at 2 of the country’s great medical schools: Tulane Medical School in New Orleans, and Washington University in St. Louis. They did their post graduate training in general surgery and medicine on the Tulane service of Charity Hospital in New Orleans. This is where they met. I also trained at Tulane Medical School and Charity Hospital 40 years later.
My mother, Dr. Jane Day, was Phi Beta Kappa in college, and Alpha Omega Alpha honor society at her medical school, Washington University in St. Louis, Missouri. She was intellectually, academically, and clinically gifted.
Unfortunately, my parents divorced when I was young. I lived with my mother, sister, and brother. I was the youngest child and grew up with a measured but keen awareness of my mother’s lifestyle and medical practice. Being the dedicated and devoted physician that she was, and possessing an unrivaled clinical acumen and gifted way of exercising it, she attracted patients from all over the state of Alabama.
Dr. Jane’s habit was to arise at 4 AM, make predawn rounds to see her patients at 3 hospitals, and then be in her office to begin treating the office patients at 7 AM. At 3 PM she left the office and made house calls, and then rounds again at the 3 hospitals. She came home around nightfall, or later. As she walked through the front door, she would call out, “John, bring in my boxes!” I would hop to it and bring in 2 or 3 boxes of patient charts from her car. These were the charts of patients she had seen that day in the office, on house calls, or in the hospitals. The boxes were stuffed with more and more patient charts as time went by, and became heavier and heavier. I would have to make 2 trips out to the car to fetch the boxes.
After arriving home, she would draw a hot bath, eat a pre-prepared supper, and then retire to her office where she efficiently dictated notes on the 2 or 3 boxes of patient charts seen that day. She went to bed around 11-12 PM.
Oftentimes she was called out at night on some kind of emergency. It seems like the house phone rang all the time. She shared call duties with a couple of other local physicians. On the back seat of the car where the boxes of patient charts were, there was a large physician’s black bag stuffed with instruments, syringes, and medicines for her house call visits. It looked just like the black bag of Dr. Felix Ittleman seen in the picture above. Sometimes her car would be broken into by people seeking drugs, and the black bag contents would become scattered about in the back seat of the car.
While driving around Montgomery, Alabama to make those house calls and hospital rounds, she would often dictate notes on charts she had in the car from that day of seeing patients. She had a wooden platform rigged up in front of the front car seat which held a small Dictaphone device so as not to squander any moments of her compressed life. She used a Dictaphone with a blue Dictabelt, exactly like this one. Once, when I was driving my own car, I saw her in her car pulling up to stop at an intersection. She was looking down at a chart and dictating. She didn’t see me watching her. A classic image and memory for me. Her automobile dictation practice never caused an auto accident.
I used to go with her on some of those house calls and hospital visits. On one house call we visited a family living in a very simple wooden structure with a red dirt floor and newspaper stuffed in wall chinks to block out drafts. On other visits we went into a finely finished homes and mansions. She treated everyone with the same kind of attention and compassion. Sometimes, when it seemed appropriate, her compassion might result in calling out the hypochondriacs and giving them a good dressing down. She might employ a lexicon of certain colorful words. Such vocalized medicine was a snapping stern reality check for those who might benefit from such guidance.
She was not one to suffer foolishness is one way of saying it. She had quite a reputation about town. Patients waiting in the front room of her office might hear her through the walls exercising her lexicon of words. She might scare some diseases right out of her patients. I became aware that this was one way of practicing mind-body medicine. I never practiced these exact techniques of my mother, but there were times over the past 50 years when I could have, and maybe I should have with a few people.
Her patients might be intimidated, but they loved her, and they kept coming back. Dr. Jane also loved her patients. There is no doubt about this. Most of her patients knew it was all mostly bluster, and they adjusted to this aspect of her ways. But it was sincere and very meaningful bluster. If you followed her admonishments, you would get better, and maybe get completely well.
Once, while riding with her on hospital rounds, I asked if she had ever saved anyone’s life. I was 12 years old. She replied in a matter-of-fact manner, “No, God does that.” That was my first, and only, verbal teaching from her. The rest of the teaching I received from her happened by way of observation and osmosis. This bit of medical wisdom has always been with me. Sometimes I would forget it, but it always came back to remind me of my true subservient role as a helper in the patient’s life process.
As her office nurse of 15 years, Nadine Johnson, used to say to me, “God did It.” Later on I added some lines to Nadine’s simple maxim to help keep me on the path of contemplation about the physician’s place in the patient’s spiritual life.
- God did It
- God does It.
- God is It.
- God was It.
Dr. Jane was a medical intuitive. She had the gift of being able to understand what was wrong with her patients not only through the clinical means in which she was well trained and practiced, but also through psychic means. She was like a CT scan before there were CT scans. When she arrived at what she thought the diagnosis was, she was sure, and ready to give treatment. And then, she got results. She was brilliant in all of this way of going about her style of post WWII medicine.
Dr. Jane retired from her 5 decades of medical practice in December, 1988. She was honored by the Alabama Senior Citizens Hall of Fame. She was selected as a Woman of Achievement in Montgomery in 1987, and honored in a banquet ceremony celebrating her and 9 other special Montgomery women. A newspaper piece claimed that she took care of an average of 12,775 patients a year, which is about 35 people a day. That seems a little rushed and compressed, but she was a whirlwind when she got going in her office, on her house calls, and on her hospital rounds. Her patients were well cared for and were never slighted in the whirlwind. She was extremely efficient in the delivery of care when so many needed it. Her patients believed in her.
My mother passed on in November, 1991, age 74, from breast cancer.
The local newspapers ran nice tributes to her. “Thousands of Montgomerians owe their health and even their lives to Dr. Jane Matthews Day, who with stern lectures and loving care doctored citizens of the area for more than 50 years…One of the first female doctors to practice in the state, Dr. Day never stopped doing house calls right up to her retirement in 1989 at the age of 71. According to friends and co-workers, she never shrank from telling patients in no uncertain terms how they needed to change their behavior. But she coupled her direct manner with a warm heart and genuine affection.”
Another newspaper article quotes one of her close friends, “‘She was one of the beloved people in Montgomery and this state’, said a close friend Baldwin Smith. ‘Her life touched more people than you can imagine.’ She was known for a tough, drill sergeant approach to medicine that was tempered by kindness and dedication. ‘She fussed like heck at patients who didn’t do what they were told. Then she would visit them at home and nurse them through all hours of the night.'”
In April, 1997, her then 112 year old 6 room office building (built in 1885), known as the Jane Day House, was moved to a site in the city devoted to preserving such Victorian houses. The laborious and tedious relocation of her office was captured and well chronicled in several local newspaper articles. Said the people responsible for the move, “Our intentions were, first and foremost, to save what we felt was an important piece of Montgomery’s history. For over 50 years, Dr. Jane Day, who was one of the first female physicians in the state, used 614 Adams Street as her office. Countless stories of this famous practitioner, from her unique diagnoses to her colorful language, have surfaced during this project, only adding to our interest in seeing the house saved.”
Said with simple unembellished no-nonsense by Dr. Jane herself, in 1988, “I just like people. I like to work. I like to work hard. I inherited that from my parents. And I inherited a certain amount of faith from them. We’re put on the earth to do something.”
Given her style of strong admonishments to her patients, you might never guess from reading those words how gifted, sensitive, and brilliant this physician was.
I went off to military school when I was 14, and my days of “bringing in the boxes” came to an end. Bringing in the boxes is a good memory and a sweet nostalgia about one little way I assisted my mother and her medicine.
On a note related to boxes of hand written charts, I retired from surgery just as “electronic medical records” was being adopted as the new accepted industry standard for how to record and document notes and plans for patients. I never used EMRs. I have hand written my notes in patient charts for the past 50 years. That amounts to a lot of contemplative chart scribing and penmanship. Writing in a patient chart adds a deeper contemplative dimension to the patient’s care, at least it does for me.
Along the way, during the days of my life and career, I have been fortunate to know and learn from many great physicians who trained in the pre and post WWII period. These physicians practiced their medicine in the style of more intimate patient contact; like what you read about in the article above, and like the way my mother practiced inside of her daily whirlwind. There were no electronic medical records or assistant office scribes tapping away on a tablet screen. Malpractice concerns had not yet blown up into the crisis that has come to haunt and influence how doctors interact with patients. The insurance companies and hospital conglomerates had not yet engulfed the frontiers of American medicine. Big Pharma and the food industry had not yet grown into the current day mercenary behemoths that they are. Robots had not appeared in operating rooms as proxies for surgeon’s hands. The advent of AI was a ways off from the scene of physician dialogue and interaction with a patient.
My interest in helping patients with their own natural healing began right around the time I entered Tulane Medical School in 1973. This interest grew over the years and came out more and more during a busy practice of general, vascular, and trauma surgery. The Haelan LifeStream model of healing in body, mind, emotions, and spirit emerged in 1999, largely out of my work with people who had cancers. I became a student of these patients and their cancer processes of disorganized cell growth; their disorganized nutrition and inner emotional and mental states; their state of spiritual connection, or not. In 2001 I stepped away from the surgery practice and began to offer lifestyle counseling. This practice continued for the next 25 years.
I think of my medical career having its beginning in my childhood apprenticeship. In the summer between my sophomore and junior year of medical school I was assisting and performing surgeries; being taught by some great physicians. Over the entire time of my medical career, I have witnessed and participated in the blossoming science based growth of holistic and integrative medicine. In December, 2000, I was a founding Diplomate of the newly formed American Board of Holistic Medicine.
At the turn of this century more and more medical schools have been offering courses for their students about natural healing. Most recently the leadership and work of Robert F. Kennedy, Jr., our Secretary of Health and Human Services, will help evolve America’s food and medical industries into better human health agencies.
All people possess a natural healing intelligence. I regard It as supreme Intelligence. It makes possible the miracle of the human body; the place where our spirit is fortunate to take birth, live, and have the incredible experience of human life. Based on my mother’s one line of teaching to me about Who It Is that does the healing, I have come to call this healing intelligence the Divine Healing Intelligence…the DHI. This DHI is driven by Divinity. It is Divinity. Perhaps the highest role of a physician is to be able to intelligently assist the DHI and not get in its way.
Physicians could be taught, and practiced, in helping their patients develop their own DHI as the main player in the proverbial black bag that each patient and each physician innately possess. This involves assisting the patient’s insight into the heart based quaternary of body, mind, emotions, spirit that they may open to and be willing to explore…meeting the physician within each person.
While we are jumping and running around chasing after our lives, we often forget that life is meant to be a spiritual experience. Some seek to know this Divinity that is our truest identity.
As the opening article above reflects, things seem like they are changing for the better as more patients and physicians want more out of their encounters with each other.
I am confident that such ways of practicing medicine offers much more to patients, and physicians, than the current styles which beg for intimacy and expanded caring.
Thanks for reading.
Signing off from Crestone and Beyond
- My Shark Story…a light hearted novelette about some events from my early teenage years which led into being tutored by a couple of great physicians during my medical school years.
- Heart Based Consciousness…a June, 2023 writing on this website about how I wandered into the mysteries of the Heart.
- Culinary Medicine is Born Anew at Tulane’s Goldring Center…a 2013 writing on this website about a novel development at my medical school; the first time an American medical school has offered a program in nutrition and cooking.
- Why Medicine Won’t Cure You (and What’s Finally Changing)…posted here on 5-11-26. A long comprehensive look at the tactics of Big Pharma, by The Midwestern Doctor. Open this link and read his opening summary of the article.
- Reclaiming the Forgotten Art of Surgery…an insightful and truly posed writing by The Midwestern Doctor, an anonymous scribe of medical truths. Here are a few summarized points: “Living tissue is immensely complex, and many spiritual traditions have provided profound insights as to what occurs when one engages in an art that interfaces with them. The art of surgery for instance is elegantly synopsized by a Chinese classic…When performing surgery, radically improves outcomes are attained as one becomes more and more able to directly connect with the body and understands precisely where to separate the tissue…Modern surgery has been overrun with new technologies (e.g. electrocautery and robotic surgery) that have been effectively marketed by their manufacturers. Unfortunately, these devices disconnect the surgeon from their patient.”
- Understanding the Foundations of Health…Dr. Joseph Mercola discusses “how true health care involves developing self-trust and personal judgment rather than blindly following medical authorities. Understanding your body’s natural healing abilities helps make informed decisions about treatments and interventions…While emergency medical care is vital for acute conditions, the current health care system often emphasizes crisis management and quick fixes rather than promoting everyday wellness and prevention…Fear disrupts self-trust and decision-making in health care choices. Developing a personal health philosophy helps you evaluate treatments based on evidence and individual experience rather than external pressure…Your body’s cellular energy production, particularly through mitochondrial health, plays a key role in overall wellness. Avoiding toxins and making lifestyle changes significantly improves natural healing capacity…Making health decisions should combine logical analysis of scientific evidence with intuitive understanding of your body. Small, consistent changes in daily habits often lead to significant health improvements.”
- The Medicalization of Death and How to Reclaim a Better Way to Die…here is a good article to ponder…”Scott Adams, who recently passed from an aggressive, rapidly progressing prostate cancer, openly shared his final journey with a wide audience, offering valuable insights for others facing the dying experience…Over centuries, the medical industry has increasingly monopolized death and dying, fostering a cultural view that treats death as something to fear, deny, and exclude from life — rather than a natural companion to accept…This distortion makes dying far more arduous in our society, fueling an escalating medicalization of death in which expensive, often futile interventions are imposed on patients — frequently against their deepest values and wishes…In contrast to the materialist scientific view that consciousness emerges solely from brain activity, compelling evidence indicates consciousness can persist independently of the brain and, in some cases, even transfer between individuals or contexts (e.g., via organ transplants or near-death accounts)…Recognizing the spiritual dimensions of dying and how they intersect with modern medical discoveries. Many ancient and enduring traditions regard this moment as one of the most significant in human life.”
- Acupuncture in the ICU–A Natural Approach to Faster Recovery…Could it be that medicine today is letting in some beneficial changes? In addition to treating the patients, I think all of the doctors and nurses and ancillary personnel in the ICUs could surely benefit as well. ICUs are high stress environments. Here are some main points raised in this article: “A mini-review published in Frontiers in Neurology suggests that acupuncture may assist ICU patients in recovering more quickly by relieving pain, lowering sedative use, shortening ventilator dependency, enhancing strength, and increasing days free from delirium…Acupuncture may help calm inflammation, boost immunity, and improve blood flow in sepsis patients, offering supportive benefits alongside standard ICU treatment…It’s not just for managing one symptom: Acupuncture could act as a whole-body support tool in the ICU, easing pain, stress, and sleep issues while reducing drug side effects and helping the body recover…Emotional Freedom Techniques (EFT) is a needle-free method using fingertip tapping on acupuncture points that offers a gentler alternative for patients wary of traditional acupuncture…Other nondrug therapies such as massage, music therapy, and mindfulness contribute to ICU recovery by alleviating anxiety, decreasing pain, and enhancing sleep quality.”
- Healthcare Decoded…an insightful video documentary on the state of healthcare in America today. ”
The United States offers some of the most advanced health care in the world, but the system is as complicated as it is incredible, making many patients feel like they are trapped in a maze. High costs, rushed care, overtreatment, and medical errors are just a few of the problems pushing our health care system to the brink of crisis…Packed full of insightful interviews with veteran medical providers, “Healthcare Decoded” lifts the veil on how the system really operates, and why it offers both the best and worst in medicine. More importantly, it provides practical tips to help you navigate this complex system.”